Cubital Tunnel Syndrome (CuTS) is a condition that occurs when the ulnar nerve, often referred to as the “funny bone” nerve, becomes compressed or irritated as it passes through the cubital tunnel on the inside of the elbow. This tunnel is a narrow passageway of bone, ligament, and muscle.
Compression of the ulnar nerve in the cubital tunnel can be caused by various factors:
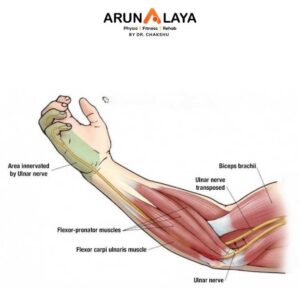
The symptoms of Cubital Tunnel Syndrome primarily affect the area supplied by the ulnar nerve, which includes the ring finger, little finger, and the ulnar side of the hand and forearm.
Common symptoms include:
Manual Therapy
Mon - Sat: 9:00AM to 8:30PM
Sunday: 9:30AM to 7:30PM
+91 8090080906
+91 8090080907
+91 8866991000