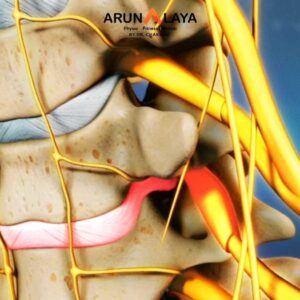
- The symptoms depend on the specific lumbar nerve root that is compressed. The most common levels for lumbar disc herniation are L4-L5 and L5-S1.
- Low Back Pain: Often localized to one side of the lower back, sometimes radiating to the buttocks. It can be dull, aching, or sharp, and may worsen with certain movements or prolonged sitting/standing.
- Radiating Leg Pain (Sciatica): The hallmark symptom of lumbar radiculopathy. Pain shoots down one leg (rarely both), often described as sharp, burning, tingling, or electric shock-like. The path of the pain follows the distribution of the affected nerve.
- Numbness or Tingling (Paresthesia): A “pins and needles” sensation or loss of feeling in specific parts of the leg or foot, corresponding to the affected nerve root (dermatomal pattern).
- Muscle Weakness: Weakness in specific muscles of the leg or foot supplied by the compressed nerve. This can lead to difficulty with walking, standing on toes/heels, or foot drop.
- Altered Reflexes: A decrease or absence of reflexes (e.g., knee jerk, ankle jerk) in the affected leg.
- Aggravating Factors: Symptoms often worsen with activities that increase intra-abdominal pressure or stretch the nerve, such as:
- Coughing, sneezing, straining (Valsalva maneuver).
- Prolonged sitting.
- Bending forward.
- Lifting.
- Straight leg raise (SLR) test is often positive.
Specific Nerve Root Involvement and Symptoms
- L4 Radiculopathy: Pain in the front of the thigh, knee. Weakness in quadriceps (knee extension). Decreased patellar reflex. Sensory loss on medial shin.
- L5 Radiculopathy: Pain in the buttock, outer thigh, lateral calf, top of the foot, and big toe. Weakness in tibialis anterior (foot dorsiflexion), extensor hallucis longus (big toe extension), gluteus medius (hip abduction), and foot evertors. Patients may have difficulty walking on heels. Sensory loss between the first and second toes.
- S1 Radiculopathy: Pain in the buttock, back of the thigh and calf, into the heel and outer foot, and little toe. Weakness in calf muscles (plantarflexion), hamstrings. Decreased Achilles reflex. Patients may have difficulty walking on toes. Sensory loss on the lateral foot.
Advanced Physiotherapy for PIVD Lumbar with Radiculopathy
- Orthopedic Tests: Including the Straight Leg Raise (SLR) test (Lasegue’s sign), crossed SLR, slump test, femoral nerve stretch test, and lumbar range of motion assessment.
- Postural and Movement Analysis: Identifying static postural deviations and dysfunctional movement patterns (e.g., guarded movements, lateral shift).
- Functional Assessment: Observing how symptoms affect walking, sitting, bending, and lifting.
Pain Management and Inflammation Control
- Activity Modification: Educating on avoiding aggravating activities and postures (e.g., prolonged sitting, heavy lifting, excessive bending/twisting).
- Modalities:-
- Cryotherapy/Thermotherapy: Ice for acute inflammation, heat for muscle relaxation.
- Transcutaneous Electrical Nerve Stimulation (TENS): For symptomatic pain relief.
- Interferential Current (IFC) or Ultrasound: May be used as adjuncts to reduce pain and inflammation.
Manual Therapy Techniques-
- Manual Lumbar Traction: Applied by the therapist to create separation between vertebrae, reducing pressure on the disc and nerve root. Can be sustained or intermittent.
- Mechanical Lumbar Traction: Using a traction unit to apply controlled, intermittent or sustained traction forces. Highly effective in creating negative pressure within the disc, promoting retraction of the herniation, and widening the neural foramen.
- Joint Mobilizations-
- Gentle Oscillatory Mobilizations: To restore segmental mobility in stiff or hypomobile lumbar and sacroiliac (SI) joints. Techniques like PA glides (central and unilateral) or transverse glides.
- Mobilization with Movement (MWM): Applied by the therapist while the patient performs an active, pain-free movement (e.g., sustained PA glide during a limited flexion movement).
Soft Tissue Mobilization-
Focusing on muscle spasms and trigger points in the paraspinal muscles, gluteal muscles, piriformis, hamstrings, and hip flexors that may be tight or guarding due to pain. Techniques include deep tissue massage, myofascial release, or instrument-assisted soft tissue mobilization (IASTM).
- Neural Mobilization (Nerve Glides):
- Gentle, controlled movements of the lower limb (e.g., straight leg raise with ankle dorsiflexion/plantarflexion) designed to mobilize the sciatic nerve or other lumbar nerve roots. This helps to reduce nerve root irritation and improve its ability to slide and glide through surrounding tissues. Performed cautiously, staying within pain-free ranges.
Therapeutic Exercise Progression
- Core Stabilization (Motor Control Exercises): Crucial for providing dynamic stability to the lumbar spine.
- Deep Abdominal Muscles: Training the transversus abdominis and multifidus (e.g., drawing-in maneuver, pelvic tilts).
- Progressive Core Strengthening: Bird-dog, planks (front and side), bridges, dead bugs, and gradually advancing to more complex core exercises.
- Lumbar Range of Motion Exercises: Gradually restoring pain-free movement in all planes (flexion, extension, lateral flexion, rotation). Often starts with directional preference exercises.
- Hip and Pelvic Strengthening: Addressing weakness in gluteal muscles (maximus, medius, minimus) and hip external rotators (e.g., clam shells, side-lying leg raises, resistance band exercises) to improve lumbopelvic stability and reduce compensatory movements.
Flexibility and Stretching
- Hamstring Stretches: Very important, as tight hamstrings can increase stress on the lumbar spine. Gentle, sustained stretches.
- Piriformis Stretches: Especially if piriformis syndrome is contributing to sciatic-like pain.
- Hip Flexor Stretches: To counter anterior pelvic tilt.
- Calf Stretches: To ensure adequate ankle dorsiflexion.
- Functional Exercises: Incorporating exercises that mimic daily activities (e.g., squatting, lunging, bending with proper form) to retrain movement patterns and improve functional capacity.
Postural and Ergonomic Education-
- Sitting Posture: Advising on lumbar support, avoiding slouching, and taking frequent breaks.
- Lifting Mechanics: Teaching proper lifting techniques using legs, keeping the load close to the body, and maintaining a neutral spine.
- Sleeping Posture: Recommending appropriate mattress firmness and pillow placement to maintain spinal alignment.
- Standing Posture: Awareness of natural spinal curves.
Return to Activity/Sport:-
- Developing a gradual and progressive return-to-activity plan, including sport-specific drills, to minimize the risk of re-injury.